Dementia
BY TALINE BOROYAN MS, OTR/L
Definitions1
Normal Aging – decrease in neurons, brain size, and brain weight. Processing and retrieval become delayed and progresses. Dementia is not a normal part of the aging process.
Types of Dementia
- Mild Cognitive Impairment
- Alzheimer’s Dementia (64%) – degenerative disease that attacks the brain and results in impaired thinking, memory, and behavior. Characterized by “plaques and tangles”
- Vascular Dementia (10%) – ischemic or hemorrhagic brain injury. Characterized by abrupt onset, focal neuro symptoms, associated cardiovascular disease. Psychological changes seen, higher incidences of depression.
- Mixed Dementia (Alzheimer’s + Vascular)
- Lewy Body Dementia – presence of Lewy Bodies in the brain. Characterized by early visuospatial impairment and gait instability.
- Parkinson’s Dementia (9% with Lewy Body) – 20-30% of people with Parkinson’s develop dementia. Characterized by physical decline followed by cognitive decline. Approximately 50% experience hallucinations.
- Fronto-Temporal Lobar Dementia (6%) – average age of onset if 57.8, frontal and temporal lobes most commonly affected. Characterized by behavioral changes.
- Normal Pressure Hydrocephalus – excess CSF accumulates in the ventricles. Characterized by memory loss, ataxia, and urinary incontinence.
- ETOH/Substance Abuse Related Dementia – continued use can cause brain damage.
*Amygdala may remain intact in many dementias (emotion center)
Clinical Implications1
All types and levels of dementia can have an impact on a person’s functional status and ability to safely care for themselves.
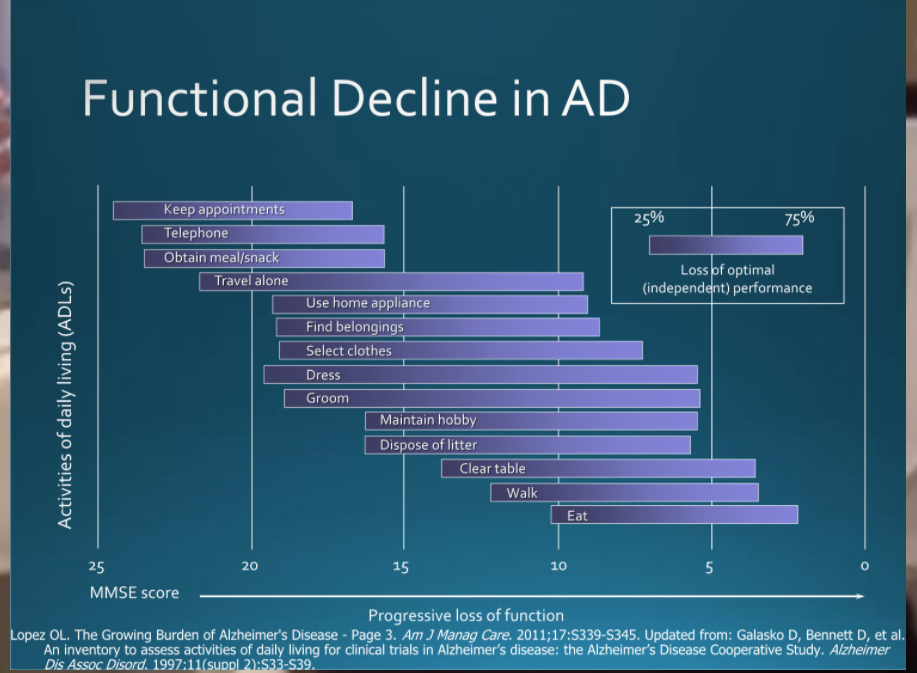
Functional Decline in Alzheimer’s Based on Mini Mental Score
Dementia is commonly associated with challenging behaviors. Behaviors can be split up into 3 parts – antecedent, behavior, consequence. Common triggers may include emotions, meds, illnesses, loss, pain, traumatic event, perceptions in their world. Best practice includes understanding the disease, understand the needs of the person, and being compassionate to their world. Recognize the loss of independence and control that they may be experiencing. Remember that behavior is communication! Think about what this person is trying to tell you as the health care provider. They may be wanting attention or affection.
Common behaviors – recognize the difference between lifelong behaviors which will not change versus new behaviors which may be able to be changed or addressed. Always consider pain as a cause.
- Resisting care
- Refusing to eat
- Yelling
- Crying
- Wandering
- Aggression and violence (i.e., hitting)
- Not sleeping
- Sundowning – burst of energy in the evening, may be related to impaired circadian rhythms
- Refusing self care (i.e., not showering)
- Inappropriate advances
Managing refusing to eat – may be due to physical factors, cognitive factors, or both. Evaluate lifelong habits, comfort food, have food events or parties, consider personal, cultural, or religious beliefs. Consults – dentist, SLP, psych, pharmacy.
Managing wandering – always approach from the front, allow it (supervised), circular pattern, talk while you walk with them, hold the persons hand, use creative techniques, only orient if the patient requests it
Managing aggression – better to distract than to reason, avoid asking open ended questions, validation therapy, reminiscence therapy (recount pleasurable experiences), sensory therapy (music therapy), pet therapy, simulated presence therapy (videos with family), always remain calm, look for patterns, be flexible
Managing delusions and hallucinations – understand if it is causing anxiety, aggression, or unwanted behaviors. Don’t contradict the belief if it is not causing harm. If it is causing harm – reassure (show listening), respond, and refocus. Consult with team to review med list!
Managing refusing self-care – elderly people get cold more easily, modesty is most likely very important to them. Gather all materials before you begin, warm setting, ask/find out bathing routine of the person, start easy with face washing, adaptive equipment (shower chair, handheld shower head).
Memory
- Remedial Approach: this is when material is organized in a logical way so that way the patient can retrieve the memory.
- Compensatory Approach: in this case there is use of a diary or notebook or other ways to remember certain skills such as calendars or beepers.
Physiotherapy emphasis: Bed mobility, transfers, gait intervention will incorporate patient education and practicing the mobility skills.
Resources
Alzheimer’s Association: https://www.alz.org/
References:
O’Sullivan, S. B., Schmitz, T. J., Fulk, G. D., & O’Sullivan, S. B. (2019). Physical rehabilitation. F.A. Davis