Wound Care
Physiology of a Wound & Wound Healing
Wound Classification:
- Acute Wound– is any surgical wound that heals by primary intention or any traumatic or surgical wound that heals by secondary intention. An acute wound is expected to progress through the phases of normal healing, resulting in the closure of the wound.
- Chronic Wound– is a wound that fails to progress healing or respond to treatment over the normal expected healing time frame (4 weeks) and becomes “stuck” in the inflammatory phase. This inflammation is due to a postponed, incomplete or uncoordinated healing process. Wound healing is delayed by the presence of many factors including medications, poor nutrition, co-morbidities or inappropriate dressing selection.
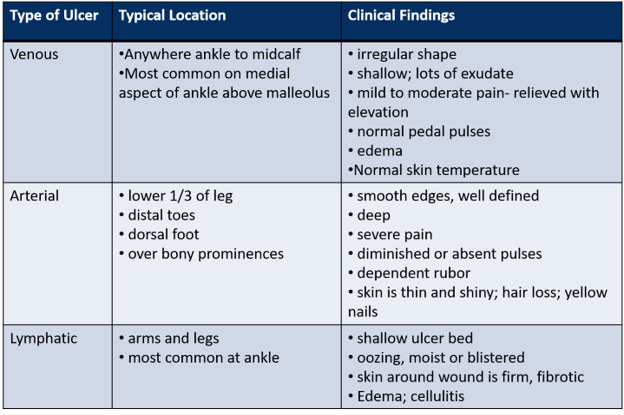
Ulcer Classification:
Type of Healing:
- Primary intention– the wound edges are held together by artificial means such as sutures, staples, tapes or tissue glue. There is minimal tissue loss and wounds heal with minimal scarring. Most clean surgical wounds and recent traumatic injuries are managed by primary closure.
- Delayed Primary Intention– when the wound is infected or requires more thorough intensive cleaning or debridement prior to primary closure (usually 3-7 days later). May be used for traumatic wounds or contaminated surgical wounds.
- Secondary Intention– spontaneous wound healing occurs through a process of granulation, contraction and epithelialization. Results in scar formation and used as a method of healing for pressure injuries or ulcers.
- Skin Graft – removal of partial or full thickness segment of epidermis and dermis from its blood supply and transplanting it to another site to speed up healing and reduce the risk of infection.
- Flap– the surgical relocation of skin and underlying structures to repair a wound. Flaps are named according to their tissue components and may include an anastomosis of blood supply to vessels attached to or at the affected site.
Wound healing is a complex sequence of events that can be broadly divided into two stages:
(A) Hemostasis – is the rapid response to physical injury and is necessary to control bleeding (stopping of blood flow). It involves the following components:
1. Vasoconstriction 2. Platelet response 3. Biochemical response
(B) Tissue Repair & Regeneration– involves 3 phases:
- Inflammation phase (0-4 Days) the body’s normal response to injury. This phase activates vasodilatation leading to increased blood flow causing heat, redness, pain, swelling and loss of function. Wound exudate may be present and this is also a normal body response.
- Reconstruction Phase (2-24 Days) the time when the wound is healing. The body makes new blood vessels, which cover the surface of the wound. This phase includes reconstruction and epithelialization. The wound will become smaller as it heals.
- Maturation phase (24 days-1 year) the final phase of healing, when scar tissue is formed. The wound is still at risk and should be protected where possible.

Factors That Inhibit Wound Healing
Holistic assessment of the patient is an important part of the wound management process. A number of local and general factors can delay or impair wound healing. These may include:
Local:
- Wound management practices- the goal is to optimize the wound environment so healing progresses
- Moisture balance- dressings are designed to promote moist wound healing
- Wound temperature and pH- a constant temperature of approximately 37’C has been shown to have a significant effect on healing along with the impact of maintaining a neutral or acidic pH to reduce the risk of bacterial colonization and opportunistic infection
- Infection- replication of organisms within a wound with subsequent host injury
- Pressure, friction and shearing, limited mobility
- Presence of foreign bodies
General:
- Underlying disease- diabetes, autoimmune disorders, anemia and malignancy. The reason these conditions impair healing include- impaired collagen, impairment of angiogenesis, delayed infiltration of inflammatory cells, macrophages and lymphocytes, due to decreased host resistance, poor cutaneous or epidermal vasculature.
- Impaired perfusion and hypoxia- cardiac conditions, smoking, shock and hemorrhage
- Malnutrition- inadequate supply of protein, carbohydrates, lipids and trace elements and vitamins essential for all phases of wound healing
- Body mass index
- Disorders of sensation or movement- cerebral palsy, movement disorders, peripheral neuropathies, spina bifida
- Medications- chemotherapy, immunosuppressive drugs, corticosteroids
- Radiation therapy
- Stress, anxiety and depression
Wound Assessment
When conducting initial and ongoing wound assessments the following considerations should be taken into account to allow for appropriate management in conjunction with the treating team:
- Type of wound- acute or chronic
- Etiology- surgical, laceration, ulcer, burn, abrasion, traumatic, pressure injury, neoplastic
- Location and surrounding skin
- Tissue Loss
- Clinical appearance of the wound bed and stage of healing
- Measurement and dimensions
- Wound edge
- Exudate
- Presence of infection
- Pain
- Previous wound management
Considerations for Wound Assessment
Type of wound: There is different terminology used to describe specific types of wounds: such as surgical incision, burn, laceration, ulcer, abrasion. They can be generally classified as either acute or chronic wounds.
Tissue loss: The degree of tissue loss may be referred to in broad terms as:
- Superficial wound– involving the epidermis
- Partial wound– involves the dermis and epidermis
- Full thickness wound-involves the epidermis, dermis, subcutaneous tissue and may extend to muscle, bones and tendons.
Wound bed clinical appearance:
- Granulating– is when healthy red tissue is observed and is deposited during the repair process. It presents as pinkish/red colored moist tissue and comprises of newly formed collagen, elastin and capillary networks. The tissue is well vascularized and bleeds easily.
- Epithelializing– is a process by which the wound surface is covered by new epithelium, this begins when the wound has filled with granulation tissue. The tissue is pink, almost white, and only occurs on top of healthy granulation tissue.
- Sloughy– the presence of devitalized yellowish tissue is observed and is formed by an accumulation of dead cells. Must not be confused with the presence of pus.
- Necrotic– describes a wound containing dead tissue. The wound may appear hard, dry and black. Dead connective tissue may appear grey. The presence of dead tissue in a wound prevents healing.
- Hyper granulating– this is observed when granulation tissue grows above the wound margin. This occurs when the proliferative phase of healing is prolonged usually as a result of bacterial imbalance or irritant forces.
Wound measurement: Assessment and evaluation of wound healing is an ongoing process. All wounds require a two-dimensional assessment of the wound opening and a three-dimensional assessment of any cavity or tracking.
- Two-dimensional assessment– can be done with a paper tape to measure the length and width in millimeters. The circumference of the wound can be traced if the wound edges are not even – often required for chronic wounds.
- Three-dimensional assessment– the wound depth is measured using a dampened cotton tip applicator.
Wound edges: The edges of the wound are assessed for:
- Color– pink edges indicate growth of new tissue; dusky edges indicate hypoxia; and erythema indicates physiological inflammatory response or cellulitis
- Evidence of contraction– wound edges coming together indicate the healing process is occurring. Raised or rolled edges- raised (where the wound margin is elevated above the surrounding tissue) may indicate hyper granulation tissue and rolled (where the edges are rolled down towards the wound bed) can inhibit healing.
- Changes in sensation– increased pain or the absence of sensation should be further investigated
Exudate: Is produced by all acute and chronic wounds (to a greater or lesser extent) as part of the natural healing process. It plays an essential part in the healing process in that it:
- Contains nutrients, energy and growth factors for metabolizing cells
- Contains high quantities of white blood cells
- Cleanses the wound
- Maintains a moist environment
- Promotes epithelialization
It is important to assess and document the type, amount, color and odor of exudate to identify any changes. Excess exudate leads to maceration and degradation of skin while too little can result in the wound bed drying out. It may become more viscous and odorous in infected wounds.
Surrounding skin: The surrounding skin should be examined carefully as part of the process of assessment and appropriate action taken to protect it from injury.
Presence of infection: Wound infection may be defined as the presence of bacteria or other organisms, which multiply and lead to the overcoming of host resistance. Infection can disrupt healing and damage tissues (local infection) or produce spreading infection or systemic illness. Infection adversely affects wound healing and may be the cause of wound dehiscence.
Local indicators of infection:
- Redness (erythema or cellulitis)
- Exudate- a change to purulent fluid or an increase in amount of exudate
- Malodor
- Localized pain
- Localized heat
- Oedema
Wound healing and clinical infection demonstrate inflammatory responses and it is important to ascertain if increases in pain, heat, oedema and erythema are related to the inflammatory phase of wound healing or infection.
If any of the above clinical indicators are present a medical review should be instigated and a Microscopy & Culture Wound Swab should be considered.
Pain: Pain can be an important indicator of abnormality. The pain associated with chronic wounds and wounds that require frequent dressing changes can be underestimated. Accurate assessment of pain is essential with regard to choice of the most appropriate dressing. Assessment of pain before, during and after the dressing change may provide vital information for further wound management and dressing selection.
REFERENCES
The Royal Children’s Hospital Melbourne. (n.d.). Retrieved March 10, 2021, from https://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Wound_assessment_and_management/
Helpful Links:
Wound Care Education Institute: Wound Care & Ostomy Educational Resources: https://www.wcei.net/resources/educational-resources
Treatment
- Scar Massage 2
- Scar Massage
- Bed Sore Prevention Program
- Ace Wrapping Transtibial Amputee
- Ace Wrapping Transtibial Amputee page 2
- Ace Wrapping Transfemoral Amputee page 2
- Acute Positioning Transfemoral Amputee
- Acute Positioning Transtibial Amputee
- Ace Wrapping Transfemoral Amputee
- OT Treatment for Pressure Ulcers
- Wound Treatment Guide
- Presentation Shrapnel Wounds
- Presentation Dressings
{kind=link}
{kind=link}