Peripheral Nerve Injuries
Peripheral nerve – A nerve belonging to the Peripheral Nervous System (PNS), a network of 43 pairs of motor and sensory nerves that connect the central nervous system (CNS, composed of the brain & spinal cord) to the entire human body
- Peripheral nerves control the functions of sensation, movement and motor coordination
- Fragile and can be damaged easily
Peripheral Nerve Injury
- Occurs when there is serious injury or trauma to one of the peripheral nerves. ● Can result in a minor injury or a fully severed nerve
- Based on the type, amount, and location of damage, nerve regeneration may or may not be possible.
Causes: Peripheral nerves can sustain injury from a number of causes, including accidents or trauma.
- Laceration (a cut or tear in the nerve tissue)
- Severe bruising (contusion)
- Gunshot wounds
- Stretching (traction)
- Drug injection injury
- Electrical injury
Symptoms
Any of the following in the the affected area
- Severe, unrelenting pain
- Burning sensation
- Tingling sensation
- Numbness sensation
- Total loss of sensation
Treatment:
Treatment depends on:
- Type of injury
- Location of injury
- The amount/severity of nerve injury sustained.
For mild nerve injuries, the following non-surgical treatments may be part of the plan: ○ Acupuncture
- Massage therapy
- Medication
- Orthotics
- Physical/occupational therapy and rehabilitation (exercises, stretches, physical agent modalities)
Classification
3 Basic Types of PNI:
- Stretch related – Most common. The peripheral nerves are elastic, but when a traction force is too strong, injury occurs. If the traction force is strong enough, a complete tear may occur, but most commonly the continuity is retained, resulting in injuries such as Erb’s Palsy.
- Lacerations – Type of injury in which the peripheral nerve is severed by a blade → Might be completely severed but usually some continuity remains.
- Compressions – Type of injury caused by excessive pressure on a nerve via nerve compression or entrapment
- Does not involve tearing of the neural elements.
- Certain nerves are more susceptible to this type of injury because of where they are located in the body
- Common entrapment neuropathies include:
- Median nerve entrapment (“Carpal tunnel syndrome”)
- Radial nerve compression (“Saturday night palsy”)
- Anterior interosseous neuropathy
- Ulnar nerve entrapment
- Femoral nerve entrapment
- Peroneal nerve entrapment
- Some medical conditions may increase the likelihood of this injury, such as diabetes, hypothyroidism, acromegaly, amyloidosis, carcinomatosis, polymyalgia rheumatica, rheumatoid arthritis or gout.
- Sunderland classification system defines five different degrees of PNI:
- First degree: A reversible local conduction block at the site of the injury. This injury does not require surgical intervention and usually will recover within a matter of hours to a few weeks.
- Second degree: There is a loss of continuity of the axons (the “electrical wires”) within the nerve. If this kind of injury can be confirmed through pre-operative nerve testing, surgical intervention is usually not required.
- Third degree: There is damage to the axons and their supporting structures within the nerve. In this case, recovery is difficult to predict. Nerve conduction studies performed during surgery are often able to help indicate outcome and need for simple cleaning of the nerve (neurolysis) or a more extensive repair with grafting.
- Fourth degree: In this case, there is damage to the axons and the surrounding tissues sufficient to create scarring that prevents nerve regeneration. Electrical testing performed during surgery confirms that no electrical energy can be passed along the neural pathways in this injured nerve. Surgical intervention with nerve grafting is necessary to repair the injury.
- Fifth degree: These injuries are usually found in laceration or severe stretch injuries. The nerve is divided into two. The only way to repair a fifth-degree injury is through surgery.
Medical Diagnosis
- In order to fully determine the extent of the damage to the nerve, the doctor may order one of the following diagnostic tests:
- An electrical conduction test to determine the passage of electrical currents through the nerves.
- Electromyography
- Nerve conduction velocity
- An imaging test such as:
- CT scan
- MRI
- MRI neurograph
- An electrical conduction test to determine the passage of electrical currents through the nerves.
UPPER & LOWER MOTOR NEURON LESIONS (UMNL & LMNL)
Clinically, we can often differentiate between upper and lower motor neuron lesions from the subjective history. For example;
- Nerve trauma, soft tissue injuries, burns, and amputation causing hypersensitivity.
- Local trauma affecting peripheral nerves such as a fibular fracture with peroneal nerve palsy or carpal tunnel syndrome, an entrapment neuropathy.
- Multiple sclerosis, stroke, or any condition impacting the central nervous system affects ascending/descending spinal tracts.
- Diabetes mellitus may cause polyneuropathy which presents with a sock/glove distribution of sensory loss.
- Lumbar disc herniation with radiculopathy causing spinal nerve entrapment.
Patient history is crucial in understanding the mechanism of injury, nature, severity of symptoms, and contributing medical conditions. Below is a table that outlines main differences between UMNL and LMNL in further detail.
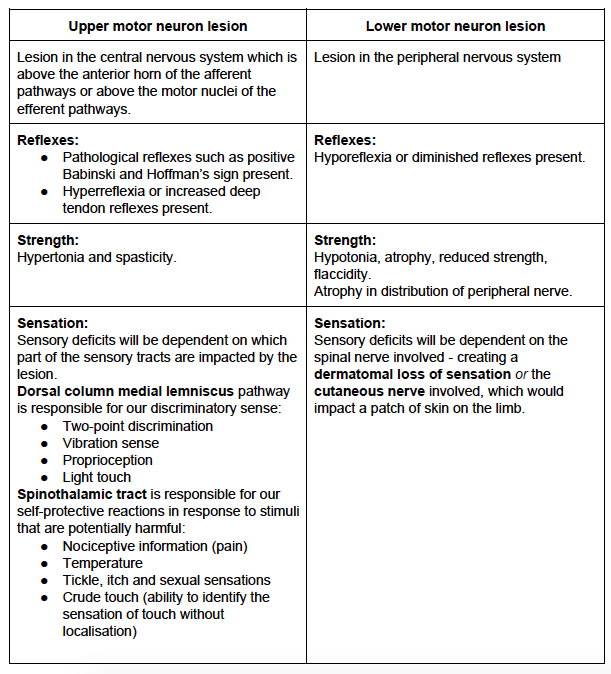
https://www.raynersmale.com/blog/2015/1/17/sensation-testing-for-person-with-peripheral-lesion
General Rehab Process:
Rehab Goals
- Prevention of secondary damage such as:
- Joint contractures
- Trophic skin damage
- Edema
- Delaying the atrophy of the affected muscles
- Stimulating the regeneration of the affected nerves or at least eliminating obstacles to regeneration.
- Compensation of the finally perished structures by:
- Strengthening of the remaining musculature
- Trick movements
- Splints or orthoses
- Surgical interventions such as muscle transplantation or muscle displacements.
- Therapeutic exercise prescription
- Initially, it serves only to maintain joint mobility and muscle length
- As soon as the first active movements are possible, try to strengthen the musculature with carefully performed resistance exercises.
- The stronger the regenerating musculature becomes, pay increased attention to continuous loading.
- Adapt the strengthening exercises to the respective stage of reinnervation.
- Strengthening can be achieved either by:
- Isolated training of the affected musculature using only slight manual resistance
- Training synergistic muscle groups, moving the paretic muscles with the help of the intact synergistic muscle groups.
- In case of severe or complete paresis, attempt to increase the tension of the muscles on the paretic side by tightening and contraction of the same muscles contralaterally
- To excite the movement of the weak muscles, use these techniques:
- Stimulation of muscle, tendons and joint receptors by pressure, tapping or stretching
- Setting of skin stimuli by brushing and thermal stimuli.
- Reduction of gravity which can be achieved by hydrotherapy (exercises in the water)
- If the affected musculature no longer achieves its original function due to the lack of reinnervation, strengthening the unaffected musculature is important in order to at least partially compensate for the missing function.
- The patients should be instructed and guided to perform independently and regularly their exercises at home
- Electrical stimulation – Can be combined with exercise therapy for pain reduction and preventing muscle atrophy
- The entire muscle should be stimulated while a significant muscle contraction occurs.
- Muscle atrophy can be slowed/prevented by regularly stimulating the denervated muscle without overstimulating or fatiguing the muscle
- Electrical muscle stimulation should be started early (if possible, a few days after the onset of the lesion) and must be performed regularly and often long (months).
Helpful websites:
About Peripheral Nerve Injury Rehabilitation
{kind=link}
Treatment
- Upper Body Peripheral Nerve Injury Interventions
- Physiotherapeutic Techniques used in the Management of Patients with Peripheral Nerve Injuries 2015
- Lower Body Peripheral Nerve Injury Interventions
- Self Rehabilitation Protocol
- Missing Attachment
- Desensitization Techniques
- Desensitization Home Program
- Home Desensitization Program
Clinical Resources
- Peripheral Nerve Lesion
- Peripheral Nervous System Pathophysiology
- Physiotherapeutic Techniques used in the Management of Patients with Peripheral Nerve Injuries 2015 1
- Peripheral Nerve Injury to the Lower Limb_ Repair and Secondary Reconstruction 2019
- Peripheral Nerve Injuries
- Rehabilitation of Peripheral Nerve Injuries 2021
- Missing Attachment