Burn Rehabilitation
Be aware of medical needs:
- Assess presence of inhalation injury and secure airway. Patients with inhalation injuries often require ventilation and intensive pulmonary hygiene.
- Chemical burns: at risk for cardiac symptoms such as arrhythmias due to the electrical current. Frequently check blood pressure, circulation, and oxygen levels. Will need frequent cleansing of damaged skin and close monitoring
- Electric burns: cause deeper, less obvious injuries that can affect vital organs and deep muscles.
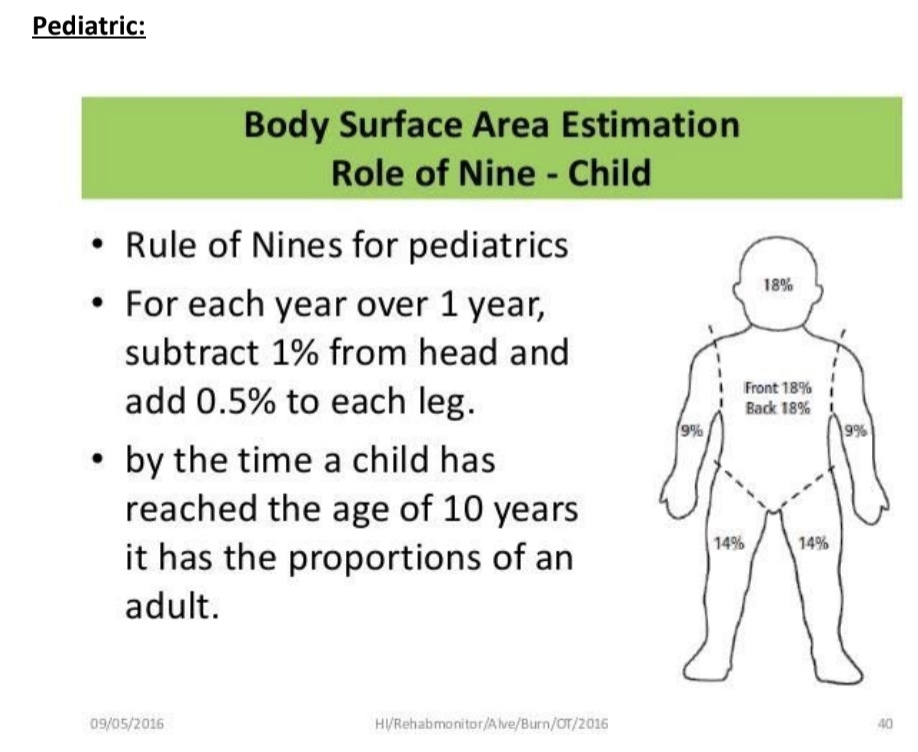
Assess the size of the burn:
- Total body Surface Area= “Rule of Nines”
- Head = 9%
- Trunk = 36%
- Upper extremity = 9% each
- Perineum = 1%
- Lower extremity = 18% each
- Burns can range from a minor injury covering 1% of a patient’s body to a severe burn covering 90%-100% of the total body surface area.
- Partial thickness burns greater than 10% of total body surface area (TBSA) require more intensive medical monitoring and intervention due to effects of significant edema. They are more likely to have mobility and movement issues and will require early PT/OT intervention.

What part of the body was burned:
- Neck and Face: Higher risk for significant edema that can cause respiratory issues, may need to be intubated for an extended period.
- Hands, feet, genitalia, perineum, or major joints: Higher risk for decreased healing, hypertrophic scarring and contractures. These parts of the body are crucial for normal function and require specialized intervention for best recovery.
- Patients who sustain full-thickness (i.e. third degree) burns are at
Assess burn depth:
| Degree of Burn | Appearance | Area affected | Sensation | Wound Closure |
| First | Pink or red, may be dry or moist, swelling, no blisters | epidermis | Intact, minimal pain | Typically heals within 3-7 days, no scarring, no skin graft |
| Second (superficial partial Thickness) | Bright pink or red, white, blisters | Epidermis and portion of dermis | Intact painful and sensitive to shance in temperature and exposure to air or touch | Heals in 7-21 days, no scarring, no skin graft |
| Second (Deep partial thickness) | Pallor, blistered, red and waxy white, wet | Epidermis and deeper portion of dermis, hair follicles, sweat glands | Variable, may be intact with areas of impaired sensations | Heals in 21-35 days or longer, scarring likely if burned over 30 % of total body surface area (TBSA), no skin graft |
| Third (full Thickness) | White or black, necrosis, dry and leathery, non pliable | Entire epidermis and dermis, hair follicles, sweat glands, nerve endings | Painless, impaired sensation; may be sensitive to deep pressure, does not feel temperature | Healing time takes months; need complex wound care, skin graft required; significantly higher risk for decreased healing, hypertrophic scarring and contractures; require nutritional support and circulation monitoring |
| Fourth | May be charred or dry | Deep soft tissues, damage to fat, muscle, and/or bone | absent | Removal of necrotic skin, skin graft required, will have hypertrophic scar; possible amputation in some cases |
Helpful websites about Burn Classifications
Rehabilitation:
- Post operative
- Focus on positioning until patient is stabilized
- Edema management
- Elevation of positioning of limbs for gravity assisted flow of edema away from extremities
- Compression: Coban or edema gloves
- Movement- rhythmic pumping
- Acute Phase: until wounds are closed
- Focus on positioning, stretching, mobility, ongoing skin assessment and scar management, education, balance, endurance, respiratory conditioning
- Compression for scar management: Ace wraps or elastic tubular bandage (e.g. Tubigrip®) use can be initiated immediately for edema control pre and post grafting
- Rehabilitative Phase: until scar maturation
- Focus on: scar management, range of motion (ROM) and stretching with techniques, mobility training as needed, education for self- management, strengthening, endurance, posture,
Rehab by burn classification
- Superficial partial thickness burn:
- Evaluate: ROM (72 hours post op); sensation (when wounds are healed), strength (when wounds are healed), ADLs and meaningful activities as soon as possible,
- Intervention: wound care, debridement, sterile whirl pool, dressing changes; gentle AROM and PROM to individual’s tolerance, edema control, splinting if necessary, ADL and role activities, minimize hypertrophic scarring, Posture/alignment during sit or stand (Asymmetries can indicate scarring)
- Deep partial thickness burns:
- Evaluate: ROM (72 hours post op); sensation (when wounds are healed), strength (when wounds are healed), ADLs and meaningful activities as soon as possible
- Intervention: wound care, debridement, sterile whirl pool, dressing changes; gentle AROM and PROM to individual’s tolerance, edema control, splinting, ADL and role activities, strengthening (when wounds are healed), minimize hypertrophic scarring, Posture/alignment during sit or stand (Asymmetries can indicate scarring)
- Full Thickness burn- requires grafting:
- Evaluate: ROM (5-7 days post-op); sensation (when wounds are healed), strength (when wounds are healed), ADLs and meaningful activities as soon as possible
- Intervention:
- 72 hours post op: dressing changes and splint at all times
- 5-7 days post op: begin AROM, light ADL and meaningful activities, sterile whirl pool
- Over 7 days: PROM as tolerated, ADL and meaningful activities
- When wounds are healed, use massage
- Minimize hypertrophic scarring, Order compression garments; Provide otoform/elastomer inserts
- Strengthening
- Posture/alignment during sit or stand (Asymmetries can indicate scarring)
Helpful Videos:
Burn Rehab- OT Eval and Treatment
References:
- Edgar, D., & Brereton, M. (2004). Rehabilitation after burn injury. BMJ (Clinical research ed.), 329(7461), 343–345. https://doi.org/10.1136/bmj.329.7461.343
- Brigham and Women’s Hospital (2008). Standard of Care: Inpatient Physical Therapy Management of Patients with Burns. Department of Rehabilitation Services Physical Therapy. Derived from www.brighamandwomens.org/assets/BWH/patients-and-families/rehabilitation-services/pdfs/inpt-burn.pdf.
- Fleming-Castaldy, R.P. (2016). Burns. TherapyEd’s National Occupational Therapy Certification Exam Review & Study Guide, by, TherapyEd, 2016, pp. 154–156.
- Trombly, L.C & Radomski, M.V (2014). Anti-Contracture Positioning by Location of Burn. Occupational Therapy for Physical Dysfunction. Wolters Kluwer/Lippincott Williams & Wilkins.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}